Stockholm syndrome, a paradoxical phenomenon, characteristic of the particular psychological functioning of people in captivity and victims of mistreatment, sexual abuse and gender-based violence, arouses significant interest in psychological sciences. However, the related instrumentation remains limited, due to the fact that there is not a significant number of measurements that can evaluate it. In addition, the current main measure (the scale for identifying “Stockholm Syndrome” reactions in young dating women/Escala para identificar reacciones de síndrome de Estocolmo (SISSR) relacionada con violencia de pareja), only exists in the English and Spanish languages; which constitutes a linguistic obstacle for its administration to individuals who speak other languages, such as French. However, the simple translation of the items of a measurement does not guarantee its reliability from a psychometric point of view. In this vein, this study proposes the translation in French and validation of the Spanish version of this measure. It also proposes, as part of testing the predictive validity of the measure, to link the construct of Stockholm syndrome with gender-related ideologies and attitudes. The validation of the French version of the Stockholm syndrome measurement scale was carried out with two samples (N = 836) consisting entirely of women. The exploratory test (EFA) carried out with 400 participants reveals a reliable tri-factorial structure of 16 elements, after the elimination of 33 elements, due to factor loadings lower than .40. The confirmatory analysis of this factorial structure, using the Structural Equation Method (CFA-SEM), carried out on a sample of 436 participants, supports the tri-factorial structure which fits the data better. Tests of factorial invariance of the measurement, depending on marital status (n1 = 215 married women; n2 = 221 concubine) reveal a structural equivalence between the groups. The predictive validity of the measure reveals that Stockholm syndrome is linked to attitudes towards gender-based violence, sexism, feminism, non-justification of the gender system and gender-based social dominance.
| Published in | Psychology and Behavioral Sciences (Volume 13, Issue 3) |
| DOI | 10.11648/j.pbs.20241303.11 |
| Page(s) | 56-74 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Stockholm Syndrome, Psychometric Assessment, Romantic Relationships, Gender-Related Ideologies, Gender-Related Attitudes
2.1. Participants
2.2. Procedure for Adapting the Stockholm Syndrome Scale in the Cameroonian Context
2.3. Measures and Procedure
2.3.1. Measures of the Exploratory Phase
2.3.2. Measures of the Confirmatory Phase
2.4. Data Analysis Procedure
3.1. Exploratory Latent Variable Analyses of the Internal Structure of the Stockholm Syndrome Scale
Three-Factors | ||||||||
|---|---|---|---|---|---|---|---|---|
Factor 1: Love-Dependence | M (SD) | EFA-FL | MSA | I-RC | Sk. | Ku. | α | ω |
1. Pour moi, mon partenaire est comme un dieu. / Para mí, mi pareja es como un dios. // For me, my partner is like a god. | 2.99 (1.82) | .85 | .86 | .63 | .46 | -.95 | .87 | .86 |
2. Sans mon partenaire, je n’ai aucune raison de vivre. /Sin mi pareja, no tengo motivos para vivir. // Without my partner, I have no reason to live. | 2.81 (1.70) | .75 | .84 | .63 | .53 | -.72 | .87 | .86 |
3. Si ma relation prend fin, je vais ressentir tellement de douleur au point de vouloir me suicider. /Si mi relación de pareja terminara, sentiría tanto dolor que querría suicidarme. // If my relationship ended, I would feel so much pain that I would want to commit suicide. | 2.66 (1.70) | .66 | .90 | .58 | .70 | -.49 | .87 | .86 |
4. Sans mon partenaire, je ne saurais pas qui je suis. /Sin mi pareja, no sabría quién soy. // Without my partner, I wouldn’t know who I am. | 2.95 (1.67) | .64 | .91 | .63 | .43 | -.73 | .87 | .86 |
5. Je ne peux pas imaginer vivre sans mon partenaire. /No puedo imaginarme viviendo sin mi pareja. // I can’t imagine living without my partner. | 2.96 (1.70) | .63 | .90 | .64 | .52 | -.55 | .87 | .86 |
Factor 2: Core (main Stockholm syndrome) | M (SD) | EFA-FL | MSA | I-RC | Sk. | Ku. | α | ω |
|---|---|---|---|---|---|---|---|---|
6. Le problème n’est pas que mon partenaire est une personne colérique, mais c’est parce que je le provoque. /El problema no es que mi pareja sea una persona enojona, sino que yo lo provoco. // The problem is not that my partner is an angry person, but that I provoke him. | 3.59 (1.68) | .65 | .90 | .49 | .05 | -.89 | .87 | .87 |
7. Mon partenaire ne se mettrait pas aussi en colère contre moi si les autres ne lui avaient pas été aussi nuisibles. / Mi pareja no se enojaría tanto conmigo si otras personas no le habrían sido tan nefastas. // My partner wouldn’t be so angry with me if other people hadn’t been so disastrous to him. | 3.69 (1.58) | .65 | .91 | .56 | -.08 | -.79 | .87 | .86 |
8. Il y a quelque chose en moi qui fait que mon partenaire perd le contrôle de sa colère. /Hay algo en mí que hace que mi pareja pierda el control de su ira. // There is something in me that makes my partner lose control of his anger. | 3.85 (1.71) | .61 | .87 | .44 | -.15 | -.84 | .87 | .87 |
9. Je ne veux pas que les autres sachent à quel point mon partenaire est en colère contre moi. /No quiero que otras personas se enteren de cuánto se enoja mi pareja conmigo. // I don’t want other people to know how angry my partner is with me. | 4.10 (1.74) | .57 | .89 | .45 | -.26 | -.91 | .87 | .87 |
10. J’aime mon partenaire, mais j’ai aussi peur de lui. /Amo a mi pareja, pero también le tengo miedo. // I love my partner, but I am also afraid of him. | 3.74 (1.77) | .53 | .90 | .48 | -.00 | -1.02 | .87 | .87 |
11. Mon partenaire n’est pas une personne violente; c’est juste qu’il perd le contrôle. / Mi pareja no es una persona violenta; es solo que pierde el control. // My partner is not a violent person; It’s just that he loses control. | 3.85 (1.85) | .49 | .90 | .48 | -.06 | -1.13 | .87 | .87 |
12. Mon partenaire est comme moi: il est aussi victime de la colère des autres. / Mi pareja es como yo, una víctima de la ira de otros. // My partner is like me, a victim of other people’s anger. | 3.94 (1.75) | .47 | .89 | .47 | -.11 | -.91 | .87 | .87 |
13. Mon partenaire est une victime autant que moi. / Mi pareja es una víctima tanto como lo soy yo. // My partner is a victim as much as I am. | 3.82 (1.75) | .45 | .88 | .41 | -.08 | -1.0 | .88 | .87 |
Factor 3: Damage (Psychological damage) | M (SD) | EFA-FL | MSA | I-RC | Sk. | Ku. | α | ω |
|---|---|---|---|---|---|---|---|---|
14. Quand je commence à être proche des gens, quelque chose de mauvais arrive. / Cuando empiezo a ser cercana con las personas, pasa algo malo. // When I start getting close to people, something bad happens. | 3.30 (1.76) | .89 | .92 | .50 | .32 | -.84 | .87 | .87 |
15. J’ai l’impression de devenir folle. / Siento como si me estuviera volviendo loca. // I feel like I’m going crazy. | 3.01 (1.74) | .74 | .77 | .51 | .50 | -.63 | .87 | .87 |
16. Je ne sais même plus qui je suis. / Ya no sé ni quien soy. // I don’t even know who I am anymore. | 2.88 (1.67) | .54 | .80 | .51 | .53 | -.55 | .87 | .87 |
χ² | Df | p-value | Factors scale | Eigenvalues | Cumulative % | Scale | ω | α |
|---|---|---|---|---|---|---|---|---|
2700.19 | 120 | < .001 | Love | 5.89 | 36.86 | Love | .88 | .88 |
Core | 1.99 | 49.33 | Core | .81 | .81 | |||
Damage | 1.29 | 57.43 | Damage | .83 | .82 | |||
SSS | .88 | .87 |
3.2. Confirmatory Factor Analyses, Scale Invariance and Evaluation of the Links Between Stockholm Syndrome and Gender Attitudes and Ideologies
3.2.1. CFA-SEM of the Structure of the Stockholm Syndrome Scale
3.2.2. Measurement Equivalence Analyses of the Stockholm Syndrome Scale (SSS) by Marital Status (Married vs. Concubine)
Model | Information criteria | Baseline test | Fit indices | Difference test | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
AIC | BIC | AIC/BIC | χ² (df) | P | CFI | ΔCFI | TLI | RMSEA [95%CI] | Δχ² | Δdf | p | |
Model 1 | 24437.12 | 24959.06 | .979 | 295.69 (176) | < .001 | .960 | .94 | .05 [.04,.06] | ||||
Model 2 | 24419.46 | 24888.39 | .981 | 304.04 (189) | < .001 | .961 | -.001 | .95 | .05 [.04,.06] | 8.34 | 13 | .82 |
Model 3 | 2442.15 | 24823.83 | .098 | 336.72 (205) | < .001 | .956 | .005 | .94 | .05 [.04,.06] | 32.68 | 16 | .008 |
Latent variables | Indicator | Concubine | Married | ||
|---|---|---|---|---|---|
Model 2 | Model 3 | Model 2 | Model 3 | ||
Factor Loadings | Mean | Factor Loadings | Mean | ||
Core | SS_C1 | 1 | 3.62 | 1 | 3.62 |
SS_C2 | 1.03 | 3.75 | 1.03 | 3.75 | |
SS_C3 | .97 | 3.94 | .97 | 3.94 | |
SS_C4 | .93 | 4.16 | .93 | 4.16 | |
SS_C5 | .87 | 3.80 | .87 | 3.80 | |
SS_C6 | 1.13 | 3.89 | 1.13 | 3.89 | |
SS_C7 | .85 | 3.98 | .85 | 3.98 | |
SS_C8 | .80 | 3.85 | .80 | 3.85 | |
Damage | SS_D1 | 1 | 3.24 | 1 | 3.24 |
SS_D2 | 1.33 | 2.99 | 1.33 | 2.99 | |
SS_D3 | 1.23 | 2.86 | 1.23 | 2.86 | |
Love-Dependence | SS_L1 | 1 | 2.92 | 1 | 2.92 |
SS_L2 | 1.06 | 2.76 | 1.06 | 2.76 | |
SS_L3 | .92 | 2.62 | .92 | 2.62 | |
SS_L4 | .96 | 2.91 | .96 | 2.91 | |
SS_L5 | 1 | 2.90 | 1 | 2.90 | |
3.2.3. Predictive Qualities of the Stockholm Syndrome Scale: Stockholm Syndrome and Gender Related Ideologies and Attitudes
(i). Empirical and Explanatory Approach to Attitudes Towards Gender-Based Violence (GBV) Through Stockholm Syndrome
(ii). Stockholm Syndrome and Sexism
(iii). Stockholm Syndrome and Adherence to Ideologies Legitimizing Gender Inequalities
(iv). Stockholm Syndrome and Feminism
| [1] | Adorjan, M., Christensen, T., Kelly, B., & Pawluch, D. (2012). Stockholm syndrome as vernacular resource. The Sociological Quarterly, 53(3), 454-74. |
| [2] | Ahmad, A., Aziz, M., Anjum, G. & Mir, F. V. (2018). Intimate partner violence and psychological distress: Mediating role of Stockholm syndrome. Pakistan Journal of Psychological Research, 33(2), 541-557. |
| [3] | Aichholzer, J., & Lechner, C. M. (2021). Refining the short Social Dominance Orientation Scale (SSDO): A validation in seven European countries. Journal of Social and Political Psychology, 9(2), 475-489. |
| [4] | Auerbach, S. M., Kiesler, D. J., Strentz, T., Schmidt, J. A., & Serio, C. D. (1994). Interpersonal impacts and adjustment to the stress of simulated captivity: An empirical test of the Stockholm syndrome. Journal of Social and Clinical Psychology, 13(2), 207-221. |
| [5] | Avina, C., & O’Donohue, W. (2002). Sexual harassment and PTSD: Is sexual harassment diagnosable trauma? Journal of Traumatic Stress, 15(1), 69-75. |
| [6] | Bachand, C., & Djak, N. (2018). Stockholm syndrome in athletics: A paradox. Children Australia, 1-6. |
| [7] | Baileya, R., Dugarda, J., Smitha, S. F., & Porges, S. W. (2023). Appeasement: Replacing Stockholm syndrome as a definition of a survival strategy. European Journal of Psychotraumatology, 14(1), 2161038. |
| [8] | Boateng, G. O., Neilands, T. B., Frongillo, E. A., Melgar-Quiñonez, H. R., & Young, S. L. (2018). Best practices for developing and validating scales for health, social, and behavioral research: A primer front. Public Health, 6, 149. |
| [9] | Bozkur, B. (2020). Developing internalized sexism scale for women: A validity and reliability study. International Journal of Eurasian Education and Culture, 5(11), 1981-2028. |
| [10] | Byrne, B. M. (1989). A primer of LISREL: Basic applications and programming for confirmatory factor analytic models. Springer-Verlag. |
| [11] | Campelli, B., Schellenberg, E. G., & Charnelle, C. Y. (1997). Evaluating measures of contemporary sexism. Psychology of Women Quarterly, 21, 89-102. |
| [12] | Cattell, R. B. (1966). The Scree test for the number of factors. Multivariate Behavioral Research, 1, 245-76. |
| [13] | Cheung, G. W., & Lau, R. S. (2012). A direct comparison approach for testing measurement invariance. Organizational Research Methods, 15(2), 167-98. |
| [14] | Cheung, G. W., & Rensvold, R. B. (2002). Evaluating goodness-of-fit indexes for testing measurement invariance. Structural Equation Modeling, 9, 233-55. |
| [15] |
Chowdhry, A. (2013). Pakistani women turn to once-taboo divorce escape abuse. Retrieved from:
http://www.reuters.com/article/uspakistan-divorce-idUSBRE90806J20130109 |
| [16] | Churchill, G. A. (1979). A paradigm for developing better measures or marketing constructs, Journal of Marketing Research, 16(1), 64-73. |
| [17] | Cronbach, L. J. (1951). Coefficient alpha and the internal structure of tests. Psychometrika, 16, 297-334. |
| [18] | de Fabrique, N., Van Hasselt, V. B., Vecchi, G. M., & Romano, S. J. (2007). Common variables associated with the development of Stockholm syndrome: Some case examples. Victims & Offenders, 2(1), 91-98. |
| [19] | Demarest, R. A. (2009). The relationship between Stockholm syndrome and post-traumatic stress disorder in battered women. Student Pulse, 1(11), 1-3. Retrieved from: |
| [20] | Dutton, D. G. & Painter, S. L. (1981). Traumatic bonding: The development of emotional attachments in battered women and other relationships of intermittent abuse. Victimology: An International Journal, 6, 139-155. |
| [21] | Dutton, D., & Painter, S. (1993). Emotional attachments in abusive relationships: A test of traumatic bonding theory. Violence and Victims, 8(2), 105-120. |
| [22] | Dzuetso Mouafo, A. V. (2024). Representations of feminism and strategies for defending male hegemony in a patriarchal context: The moderating effect of sociodemographic and attitudinal variables. International Journal of Psychological Science, 4(1), 9-20. |
| [23] | Dzuetso Mouafo, A. V. (2024). Domestic violence experienced by women: Construction and validation of a measurement method. International Journal of Psychological Science, 4(2), 21-31. |
| [24] | Dzuetso Mouafo, A. V., & Ekango Nzekaih, H. K. (2021). Gender system justification, gender differences and attitudes towards women’ victimization. Social Sciences, 10(2), 67-73. |
| [25] | Dzuetso Mouafo, A. V., & Nzeuta Lontio, S. (2022). Confirmatory factor structure assessment of the French version of the Femininity Ideology Scale. Psychology and Behavioral Sciences, 11(6), 201-210. |
| [26] |
Fonseca, N. Q. L., & Oliveira, B. Q. (2021). Liaison traumatique: Concepts, causes et mécanismes dans les relations intimes [Traumatic liaison: Concepts, causes and mechanisms in intimate liaisons]. Revista Científica Multidisciplinar Núcleo do Conhecimento, 6, 60-78.
https://www.nucleodoconhecimento.com.br/psychologie-fr/liaison-traumatique |
| [27] | George, V. (2015). Traumatic bonding and intimate partner violence [Master’s thesis, University of Wellington]. |
| [28] | Graham, D. L. (1994). Loving to survive: Sexual terror, men’s violence, and women’s lives. New York University Press. |
| [29] | Graham, D. L. R., Rawlings, E. I., Ihms, K., Latimer, D., Foliano, J., Thompson, A., Suttman, K., Farrington, M., & Hacker, R. (1995). A scale for identifying “Stockholm Syndrome” reactions in young dating women: Factor structure, reliability, and validity. Violence and Victims, 10(1), 3-22. |
| [30] | Hu, L., & Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling: A Multidisciplinary Journal, 6(1), 1-55. |
| [31] | Hurley, K. J., & Morganson, V. J. (2022). An empirical examination of sexual harassment and Stockholm syndrome in relation to essential and non-essential workers during the COVID-19 pandemic. Journal of Sexual Aggression, 29(2), 1-13. |
| [32] | Jameson, C. (2010). The short step from love to hypnosis: A Reconsideration of the Stockholm syndrome. Journal for Cultural Research, 14(4), 337-355. |
| [33] | Jöreskog, K. G., & Sörbom, D. (2004). LISREL 8.54. Structural Equation Modeling with the Simplis Command Language. |
| [34] | Josse, E. (2022). Le syndrome de Lima, reflet en miroir du syndrome de Stockholm [Lima syndrome, a mirror image of Stockholm syndrome]. Retrieved from: |
| [35] |
Josse, E. (2022). Un nouveau regard sur le syndrome de Stockholm [A new look at Stockholm syndrome]. Retrieved from:
https://www.resilience-psy.com/un-nouveau-regard-sur-le-syndrome-de-stockholm/ |
| [36] | Jülich, S. (2005). Stockholm syndrome and child sexual abuse. Journal of Child Sexual Abuse: Research, Treatment, & Program Innovations for Victims, Survivors, & Offenders, 14(3), 107-129. |
| [37] | Jülich, S. (2013). Stockholm syndrome and sex trafficking: Why don’t they do something? Fair Observer. Retrieved from: |
| [38] | Kaiser, H. F. (1974). An index of factorial simplicity. Psychometrika, 39(1), 31-36. |
| [39] | Karan, A., & Hansen, N. (2018). Does the Stockholm syndrome affect female sex workers? The case for a “Sonagachi Syndrome”. International Health and Human Rights, 18, 10. |
| [40] |
Kearney, A., & Muñana, C. (2020). Taking stock of essential workers. Retrieved from:
https://www.kff.org/policy-watch/taking-stock-ofessential-workers/ |
| [41] | Khairaat, N., Murdiana, S., & Nur, H. (2023). Kecenderungan Stockholm syndrome pada perempuan korban kekerasan dalam berpacaran di kota Makassar [The tendency of Stockholm syndrome in women victims of dating violence in the city of Makassar]. Jurnal Pendidikan, Sosial dan Humaniora, 2(3), 484-491. |
| [42] | Kirby, S., Greaves, L., & Hankivsky, O. (2000). The dome of silence: Sexual harassment and abuse in sport. Fernwood Publishing. |
| [43] |
Kitroeff, N. (2012). Stockholm syndrome in the pimp-victim relationship. Retrieved from:
https://kristof.blogs.nytimes.com/2012/05/03/stockholm-syndrome-in-the-pimp-victim-relationship/. |
| [44] | Kline, R. B. (2016). Principles and practice of structural equation modeling. Guilford Press. |
| [45] | Kouassi, A. M., & Bissouma, A.-C. (2023). Cognitive distortions and coping strategies: Stockholm syndrome among victims of assault in Ivory Coast. European Journal of Humanities and Social Sciences, 3(6), 1-13. |
| [46] |
Krug, E. G., Dahlberg, L. L., & Mercy, J. A. (2002). World report on violence and health. Retrieved from:
http://apps.who.int/iris/bitstream/10665/42495/1/9241545615_eng.pdf |
| [47] | McDonald, R. P. (1999). Test theory: A unified treatment. Lawrence Erlbaum Associates Publishers. |
| [48] | Namnyak, M., Tufton, N., Szekely, R., Toal, M., Worboys, S., & Sampson, E. L. (2008). ‘Stockholm syndrome’: Psychiatric diagnosis or urban myth? Acta Psychiatrica Scandinavica, 117(1), 4-11. |
| [49] | Nunnally, J. C. (1978). Psychometric Theory. McGraw-Hill. |
| [50] | Peirce, E. R., Rosen, B., & Hiller, T. B. (1997). Breaking the silence: Creating user-friendly sexual harassment policies. Employee Responsibilities and Rights Journal, 10(3), 225-242. |
| [51] | Raykov, T., & Marcoulides, G. A. (2011). Introduction to Psychometric Theory. Routledge. |
| [52] | Rizo Martínez, L. E. & Santoyo Telles, F. (2019). Traducción al español y validación de la escala para identificar reacciones de síndrome de estocolmo (sissr) relacionada con violencia de pareja en mujeres mexicanas. Revista Argentina de Clínica Psicológica, 29(5), 849-858. |
| [53] | Rosseel, Y. (2012). Lavaan: An R package for structural equation modeling. Journal of Statistical Software, 48(2), 1-36. |
| [54] | Selič, M. (2016). The phenomenon of Stockholm syndrome in abusive relationships. Retrieved from: |
| [55] | Strentz, T. (1980). The Stockholm syndrome: Law enforcement policy and ego defenses of the hostage. Annals of the New York Academy of Sciences, 347(1), 137-150. |
| [56] | Vandenberg, R. J., & Lance, C. E. (2000). A review and synthesis of the measurement invariance literature: Suggestions, practices, and recommendations for organizational research. Organizational Research Methods, 3(1), 4-70. |
| [57] | Verniers, C., & Martinot, D. (2015). L’EJSAG, une échelle de justification du système spécifique au genre: Validation auprès d’une population d’adolescents et d’adultes. L’année psychologique/Topics in Cognitive Psychology, 115, 107-140. |
| [58] | Yoshihama, M., Bybee, D., Dabby, C., & Blazevski, J. (2011). Lifecourse experiences of intimate partner violence and help-seeking among Filipina, Indian, and Pakistani women: Implications for justice system responses. Retrieved from: |
| [59] | Yoshioka, M. R., Dinoia, J., & Ullah, K. (2002). Attitudes towards marital violence: An examination of four Asian communities. Violence Against Women, 7, 900-926. |
| [60] | Zakar, R., Zakar, M. Z., & Krӓmer, A. (2011). Spousal violence against women in the context of marital inequality: Perspectives of Pakistani religious leaders. International Journal of Violence and Conflict, 5, 317-384. |
APA Style
Mouafo, A. V. D., Lontio, S. N. (2024). Stockholm Syndrome and Gender-Related Ideologies and Attitudes: A Psychometric Assessment. Psychology and Behavioral Sciences, 13(3), 56-74. https://doi.org/10.11648/j.pbs.20241303.11
ACS Style
Mouafo, A. V. D.; Lontio, S. N. Stockholm Syndrome and Gender-Related Ideologies and Attitudes: A Psychometric Assessment. Psychol. Behav. Sci. 2024, 13(3), 56-74. doi: 10.11648/j.pbs.20241303.11
AMA Style
Mouafo AVD, Lontio SN. Stockholm Syndrome and Gender-Related Ideologies and Attitudes: A Psychometric Assessment. Psychol Behav Sci. 2024;13(3):56-74. doi: 10.11648/j.pbs.20241303.11
@article{10.11648/j.pbs.20241303.11,
author = {Achille Vicky Dzuetso Mouafo and Sylvestre Nzeuta Lontio},
title = {Stockholm Syndrome and Gender-Related Ideologies and Attitudes: A Psychometric Assessment
},
journal = {Psychology and Behavioral Sciences},
volume = {13},
number = {3},
pages = {56-74},
doi = {10.11648/j.pbs.20241303.11},
url = {https://doi.org/10.11648/j.pbs.20241303.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.pbs.20241303.11},
abstract = {Stockholm syndrome, a paradoxical phenomenon, characteristic of the particular psychological functioning of people in captivity and victims of mistreatment, sexual abuse and gender-based violence, arouses significant interest in psychological sciences. However, the related instrumentation remains limited, due to the fact that there is not a significant number of measurements that can evaluate it. In addition, the current main measure (the scale for identifying “Stockholm Syndrome” reactions in young dating women/Escala para identificar reacciones de síndrome de Estocolmo (SISSR) relacionada con violencia de pareja), only exists in the English and Spanish languages; which constitutes a linguistic obstacle for its administration to individuals who speak other languages, such as French. However, the simple translation of the items of a measurement does not guarantee its reliability from a psychometric point of view. In this vein, this study proposes the translation in French and validation of the Spanish version of this measure. It also proposes, as part of testing the predictive validity of the measure, to link the construct of Stockholm syndrome with gender-related ideologies and attitudes. The validation of the French version of the Stockholm syndrome measurement scale was carried out with two samples (N = 836) consisting entirely of women. The exploratory test (EFA) carried out with 400 participants reveals a reliable tri-factorial structure of 16 elements, after the elimination of 33 elements, due to factor loadings lower than .40. The confirmatory analysis of this factorial structure, using the Structural Equation Method (CFA-SEM), carried out on a sample of 436 participants, supports the tri-factorial structure which fits the data better. Tests of factorial invariance of the measurement, depending on marital status (n1 = 215 married women; n2 = 221 concubine) reveal a structural equivalence between the groups. The predictive validity of the measure reveals that Stockholm syndrome is linked to attitudes towards gender-based violence, sexism, feminism, non-justification of the gender system and gender-based social dominance.
},
year = {2024}
}
TY - JOUR T1 - Stockholm Syndrome and Gender-Related Ideologies and Attitudes: A Psychometric Assessment AU - Achille Vicky Dzuetso Mouafo AU - Sylvestre Nzeuta Lontio Y1 - 2024/05/10 PY - 2024 N1 - https://doi.org/10.11648/j.pbs.20241303.11 DO - 10.11648/j.pbs.20241303.11 T2 - Psychology and Behavioral Sciences JF - Psychology and Behavioral Sciences JO - Psychology and Behavioral Sciences SP - 56 EP - 74 PB - Science Publishing Group SN - 2328-7845 UR - https://doi.org/10.11648/j.pbs.20241303.11 AB - Stockholm syndrome, a paradoxical phenomenon, characteristic of the particular psychological functioning of people in captivity and victims of mistreatment, sexual abuse and gender-based violence, arouses significant interest in psychological sciences. However, the related instrumentation remains limited, due to the fact that there is not a significant number of measurements that can evaluate it. In addition, the current main measure (the scale for identifying “Stockholm Syndrome” reactions in young dating women/Escala para identificar reacciones de síndrome de Estocolmo (SISSR) relacionada con violencia de pareja), only exists in the English and Spanish languages; which constitutes a linguistic obstacle for its administration to individuals who speak other languages, such as French. However, the simple translation of the items of a measurement does not guarantee its reliability from a psychometric point of view. In this vein, this study proposes the translation in French and validation of the Spanish version of this measure. It also proposes, as part of testing the predictive validity of the measure, to link the construct of Stockholm syndrome with gender-related ideologies and attitudes. The validation of the French version of the Stockholm syndrome measurement scale was carried out with two samples (N = 836) consisting entirely of women. The exploratory test (EFA) carried out with 400 participants reveals a reliable tri-factorial structure of 16 elements, after the elimination of 33 elements, due to factor loadings lower than .40. The confirmatory analysis of this factorial structure, using the Structural Equation Method (CFA-SEM), carried out on a sample of 436 participants, supports the tri-factorial structure which fits the data better. Tests of factorial invariance of the measurement, depending on marital status (n1 = 215 married women; n2 = 221 concubine) reveal a structural equivalence between the groups. The predictive validity of the measure reveals that Stockholm syndrome is linked to attitudes towards gender-based violence, sexism, feminism, non-justification of the gender system and gender-based social dominance. VL - 13 IS - 3 ER -
Department of Philosophy and Psychology, University of Maroua, Maroua, Cameroon
Department of Philosophy-Psychology-Sociology, University of Dschang, Dschang, Cameroon
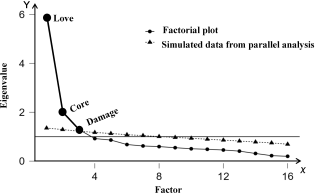
Figure 1. Scree graph.
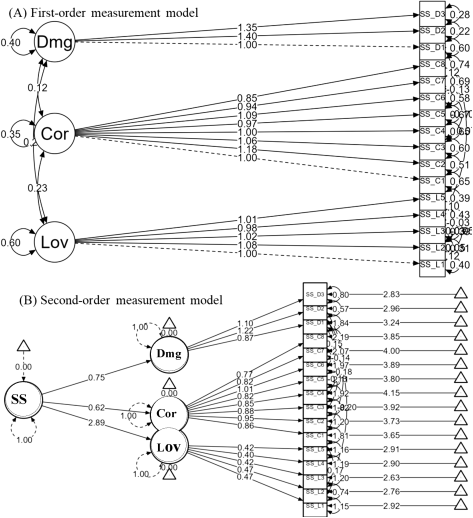
Figure 2. First and second-order confirmatory tri-factor structures (CFA) of the Stockholm syndrome scale.
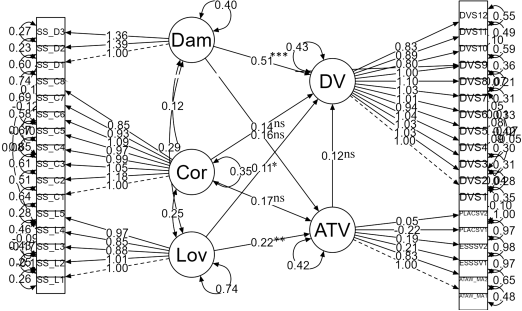
Figure 3. Evaluations of structural relationships between Stockholm syndrome, attitudes towards gender-based violence and experienced domestic violence.
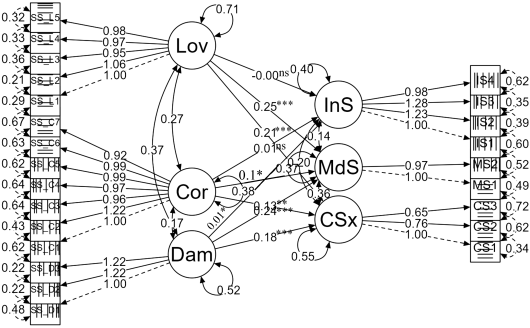
Figure 4. Structural model predicting attitudes towards sexism through Stockholm syndrome.
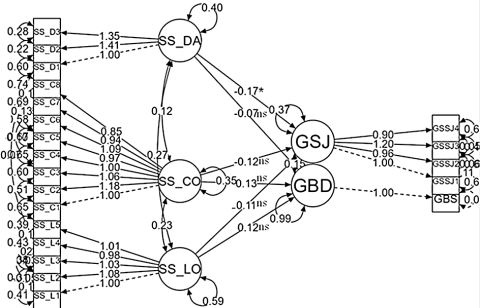
Figure 5. Explanatory model of adherence to ideologies legitimizing gender inequalities through Stockholm syndrome.
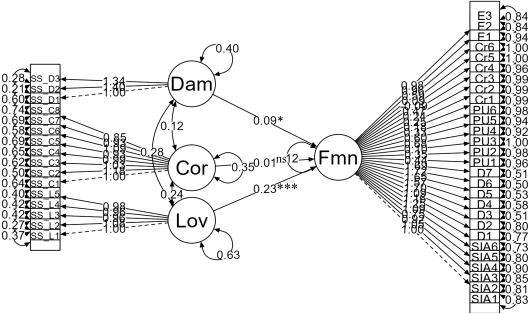
Figure 6. Analysis of the structural relationships between Stockholm syndrome and feminist ideology.

